


Autism, Food Sensitivity, and Gastrointestinal Candidiasis
An autism case study using antifungal therapy and dietary intervention - Medical Academy of Pediatric Special Needs (MAPS) - part 5

In January 2010 an article by W. Shaw, et. al. titled “Immunodeficiency, Gastrointestinal Candidiasis, Wheat and Dairy Sensitivity, Abnormal Urine Arabinose, and Autism: A Case Study” was published in the North American Journal of Medicine and Science. This 7-page article detailed significant findings related to gastrointestinal candidiasis, benefits of a gluten and casein-free (GFCF) diet, and antifungal therapy. In less than a half-year of therapy the child went from a Childhood Autism Rating Scale (CARS) of 43 (severely autistic) to 29 (non-autistic). For a more detailed accounting of this child’s case and subsequent discussion, including references, make sure to access the full article HERE.
What follows are some important details from this article.
Introduction
Most children with autism have substantial immune abnormality of some type
There is a high correlation between the prevalence of ear infections and the incidence of autism. The earlier a child has an ear infection, the more likely that child has a severe form of autism.
Arabinose, a type of sugar, is associated with candida infection and may be a consequence of frequent antibiotic use. Previous case reports show arabinose, and other urine fungal metabolites, decrease after antifungal therapy along with symptoms of autism.
Candida infection is also common in children with immune deficiencies who do not have an unusually high number of infections treated with antibiotics.
Case Report of 5-Year-Old Caucasian Male w/Autism
Normal birth at term and normal apgar scores
Newborn metabolic screening, i.e., phenylketonuria, within normal limits
At 16 months the boy had surgery for a blocked tear-duct and possible undescended testicle. He was put on prophylactic antibiotics after surgery.
Up to age of three years the boy had one or two ear infections treated with antibiotics, a couple of colds, and an upper respiratory infection.
Immunizations were all on schedule
At 15 months of age he was assessed by pediatrician and deemed normal developmentally, despite some concerns expressed by parents regarding his lack of speech.
Measles, Mumps, and Rubella (MMR) vaccine was administered at 18 months, and pediatrician noted “does not need to return until 2 years of age.” No recommendations given regarding lack of speech.
At his 2-year and 2.5-year follow-up appointments his lack of expressive language was noted, and finally child was referred to a hearing and speech clinic for assessment. His hearing assessment was normal.
His diet consisted of bread, pancakes, milk, peanut butter, and chicken. It was noted by pediatrician that he always had loose stools.
Because of lack of expressive language, a developmental assessment was done at 27 months in which the boy was diagnosed autistic with a developmental age between 19-20 months.
At his developmental assessment consultation appointment he was diagnosed with an ear infection and antibiotics prescribed.
No testing was done to assess immune or gastrointestinal function
At about 3-years of age, the parents pursued additional biochemical assessment, including allergies, blood chemistry and immune status, stool analysis, and urine organic acids test (OAT).
Results of these tests revealed the following:
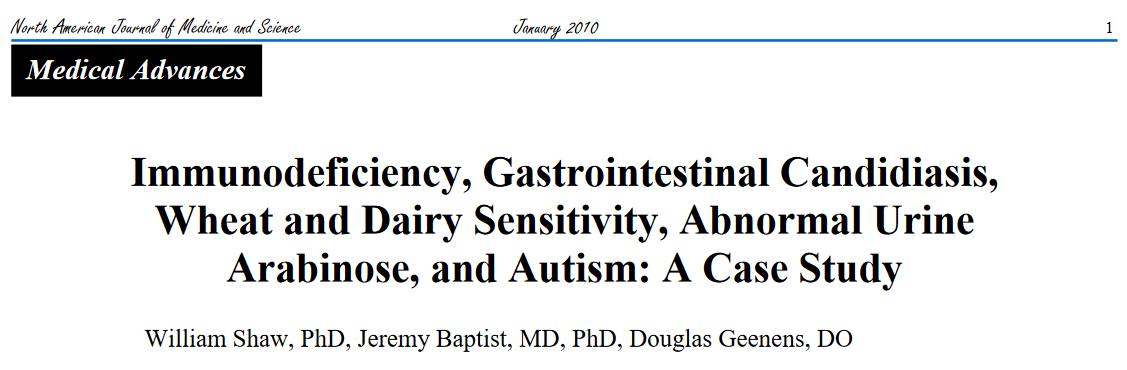
Extremely low serum IgA (Table 1)

Image 1 - Notice all immunoglobulins are normal, including IgG1-4 subclasses, except for IgA. IgA deficiencies occur in approximately 1 in 700 people and can lead to low secretory IgA production compromising mucosal immunity.
4+ overgrowth of Candida parasilosis on stool testing (sensitivity was positive to fluconazole, itraconazole, nystatin, and ketoconazole).
Gamma-streptococci (3+) and hemolytic E. coli (4+) were also detected on stool testing, along with Lactobacillus and Bifidobacterium at 3+ and 4+, respectively.
His organic acids test showed showed high levels of sugar arabinose
A comprehensive food allergy test was performed showing high IgG antibodies to barley, gluten, wheat, bran, cow’s milk, cheeses, beef, grapefruit, orange, peanut, soybean, and sugar.
An endomysial antibody test specific for celiac disease was negative
Other blood chemistry testing was normal, except for low white blood cell count, and a slight elevation of atypical lymphocytes.
What follows is a outline of this child’s therapy and therapeutic intervention results. It’s important to remember that the positive changes to this child’s condition manifested over less than a 6 month period of time. In conventional medicine there are no available or recognized autism treatments that show these kinds of results:
Child was placed on 100,000 units of Nystatin four times daily. Nystatin was alternated with a week of Nizoral or Diflucan (2mg/kg) as well.
After two months of antifungal therapy he was placed on a gluten-free and casein-free (GFCF) diet.
Both the diet and antifungal therapies were used for about 6 months, but urine organic acids testing was completed after 4 months showing an arabinose reduction from 341 mmol/mol creatinine (14X the mean value) to 51 mmol/mol creatinine which is still elevated compared to normal controls, but significantly less. An additional two months brought the arabinose down to 29 mmol/mol creatinine which was aligned with mean value of 24.1 mmol/mol creatinine of neurotypical children.
A follow-up stool analysis showed complete absence of candida
Results of the antifungal therapeutic intervention are as follows:
Significant increase in eye contact
Significant decrease in self-stimulatory behavior
Increased use of spontaneous language
With regards to notable changes following the initiation of a GFCF diet:
Mother reports child able to follow three-step verbal directions versus only one step directions previously.
Increased learning speed in school
Increased verbal labeling
Increased spontaneous verbal initiations
The child’s CARS score dropped from a high of 43 (severely autistic) to 29 (non-autistic) after therapy. The cutoff CARS score for autism is 30 or above.
The child was reassessed by a state university autism clinic and was found to be a high-functioning individual with autism. His play was parallel with other children in class, and he demonstrated interest in peers, toy sharing, and imaginative play.
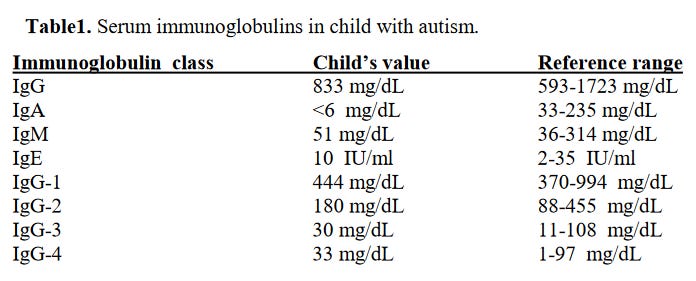
Table 2 below shows the before and after Candida parapsilosis on stool test, arabinose on organic acids test, and CARS scores.
Image 2 - Only after 4 months of antifungal therapy the stool analysis was normal for Candida parapsilosis, relatively the same arabinose as neurotypical controls, and a normal CAR score.
The immunodeficiency model for autism outlined in this article shows the connections between poor immunity, chronic infections from fungus, immunotoxins, and other toxic compounds such as pentosidine formation and subsequent neurological damage. Interestingly, chronic yeast overgrowth in the intestines is linked to hypoglycemia and ketosis, and may contribute to impaired brain function.

Image 3 - Arabinose is an aldehyde compound that can cause various adverse reactions, including pentosidine formation. Gliotoxin is linked to yeast overgrowth (specifically candida), but this toxin is a known compound produced by certain aspergillus spp. too. Gliotoxin inhibits immune function, and can damage mitochondria.
Genetic immunodeficiencies may play a role in some cases of autism. For example, a myeloperoxidase deficiency linked to a defect in this enzymes production leads to inability to kill fungus. There are other documented abnormalities in autism that include:
IgG deficiency
IgA deficiency
IgG subclass deficiency
Reduced natural killer cell activity
Elevated cytokines like IL-12 and interferon-gamma linked to neuroinflammation
Positive anti-myelin antibodies
Positive anti-serotonin antibodies
Complement C4b deficiency
Finally, some immune abnormalities in autism have been linked to adverse reactions to vaccinations. The authors mention (along with references) “measles vaccination, even as a dose of single vaccine, has been shown to specifically induce cellular immune deficiency to Candida in the majority of infants vaccinated.”